Oregon Must Choose Early Childhood Investments for a Better Future
Governor Kotek released her Recommended Budget for 2025-27 on Monday, December 2. While it makes some notable needed investments in young children, more is needed to ensure Oregon lives up to our values of supporting young children and families furthest from opportunity. These investments help families overcome generational poverty, put working families on a path to success, and strengthen the state’s economy.
The Governor’s Recommended Budget recognizes the need to start early with some small but important investments.
Existing Early Childhood Investments
- $12.7 million to provide early childhood mental health consultation support to child care providers experiencing challenging behaviors in their classrooms. This is a $4.4 million increase from 2023-25.
- $19.6 million to continue the work of the Birth to 5 Early Literacy Fund for the 2025-27 biennium, and $2.2 million for Imagination Library.
- $4.7 million investment in the new Tribal Early Learning Fund.
We are calling on the legislature to go further with three targeted investments for young children and families living in poverty that strengthen both our early childhood and economic ecosystems across this state, especially in rural areas.
Strategic Investments for 2025-2027
- Employment Related Day Care: $500 million is needed to reach unconnected and waitlisted families. More than 8,000 families are on a waitlist to access help to pay for child care. This means parents can’t work and provide for their families. Child care shortages hinder our economy and the ability of employers to recruit and retain workers.
- Momnibus Package: Pass needed legislation and allocate at least $20 million. Rep. Lisa Reynolds has spent months working with partners to develop a Momnibus package of investments focused on stabilizing families during pregnancy and the first year of a child’s life. Prioritize the passage of the Momnibus package and approximately $20 million needed for implementation.
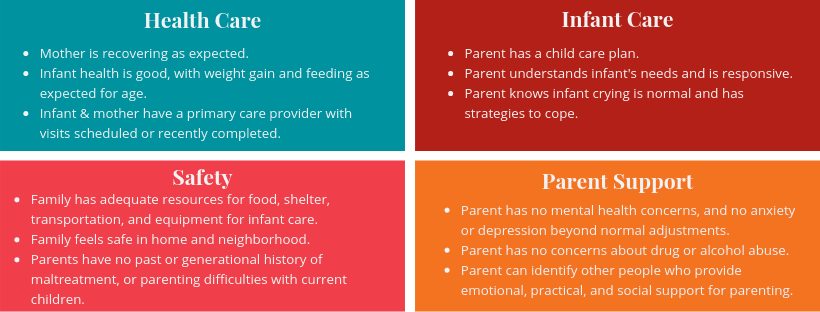
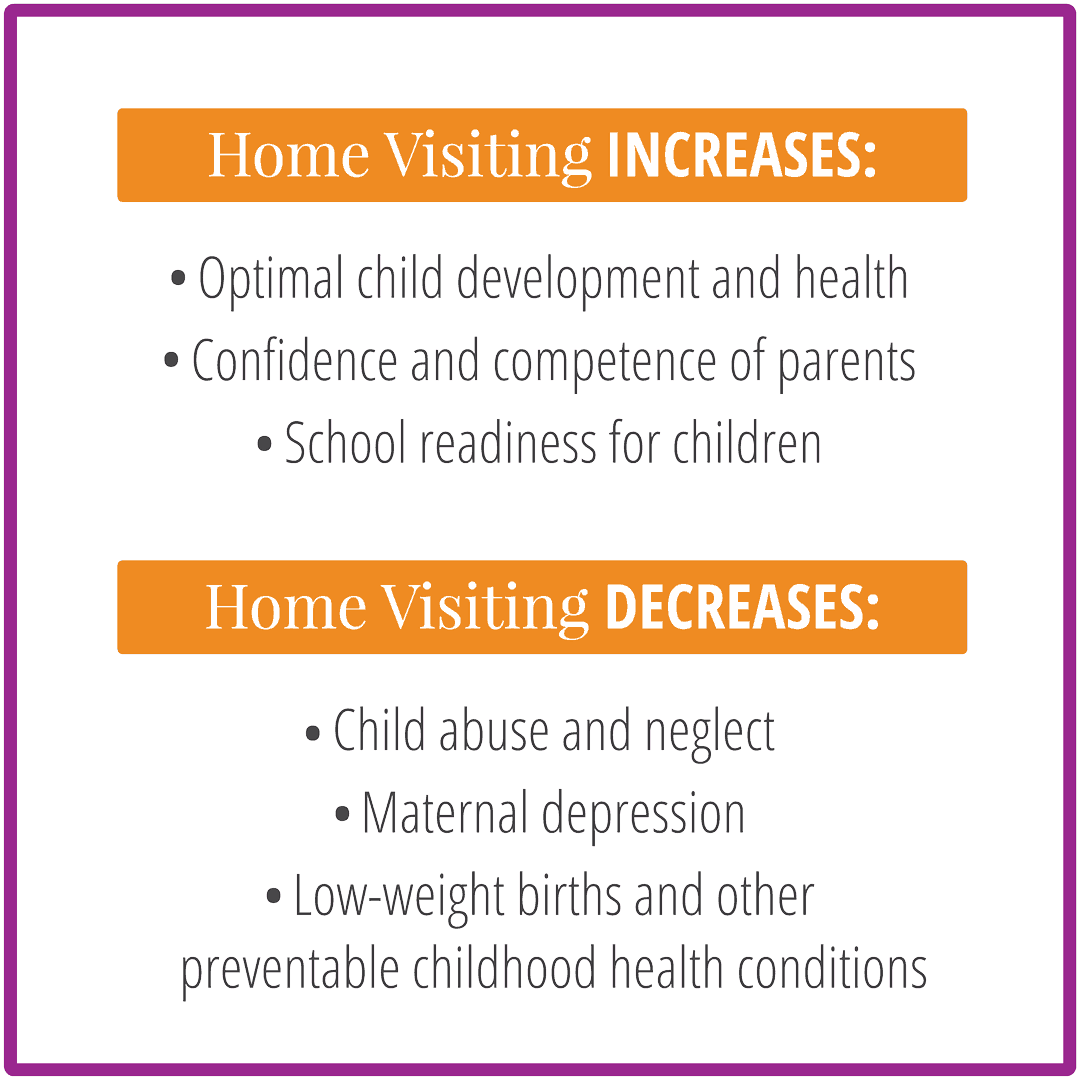
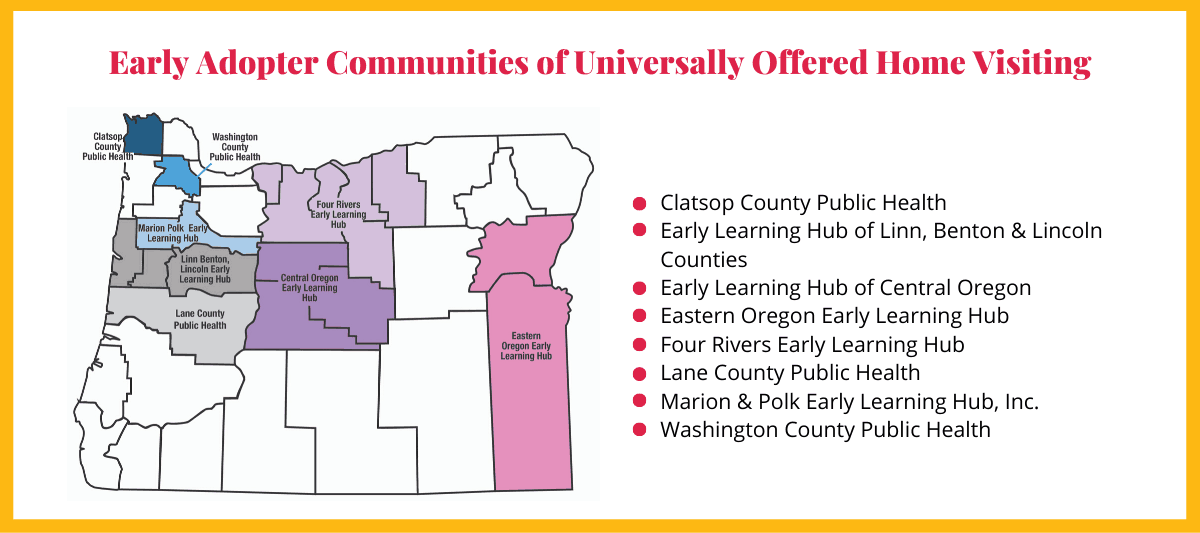
- Home Visiting: $26 million investment. Breaking intergenerational cycles of trauma requires investments that support families. Home visiting programs strengthen healthy child development and school readiness while helping prevent child abuse and maternal depression. These are crucial services for families raising our youngest Oregonians.
Early childhood investments yield some of the best returns for any public funding and have broad public support. We call on Governor Kotek and the Oregon Legislature to make these choices today for a much brighter and stronger future for the state.
We Need You!
While you’re here, please sign our petition to help elevate the importance of early childhood investments in the legislature in 2025. It takes 10 seconds and your name makes a difference!